![[in]genios](http://images.squarespace-cdn.com/content/v1/51c861c1e4b0fb70e38c0a8a/48d2f465-eaf4-4dbc-a7ce-9e75312d5b47/logo+final+%28blanco+y+rojo%29+crop.png?format=1500w)
Estudio de caso sobre los efectos de la migración circular en los niveles de glucosa de un paciente con diabetes tipo 2
DOI: https://doi.org/10.54114/ingeniosv12i2.12618
Camila S. Vásquez Vidal
Departamento de Biología
Facultad de Ciencias Naturales, UPR RP
Recibido: 19/09/2025; Revisado: 17/02/2026; Aceptado: 20/03/2026
Abstract
Type 2 diabetes mellitus (T2DM) disproportionately affects Hispanic/Latino populations, including Puerto Ricans. This exploratory case study evaluated whether circular migration between Puerto Rico and El Salvador influenced fasting glucose levels in a single individual. A 64-year-old man with T2DM was monitored over two 14-day periods, recording glucose, diet, physical activity, weight, and medication use. Mean fasting glucose was significantly lower in El Salvador than in Puerto Rico (123.6 vs 172-.6 mg/dL; p = 0.0006), despite discontinuation of metformin, and coincided with higher step counts. Macronutrient intake was similar. These findings suggest lifestyle factors, particularly physical activity, influence glycemic control.
Keywords: type 2 diabetes mellitus, glycemic variability, migration, health
Resumen
La diabetes mellitus tipo 2 (DM2) afecta de manera desproporcionada a las poblaciones hispanas, incluidos los puertorriqueños. Este estudio exploratorio evaluó si la migración circular entre Puerto Rico y El Salvador se asocia con cambios en la glucosa en ayunas en un mismo individuo. Se observó a un hombre de 64 años durante dos periodos de 14 días, registrando glucosa, dieta, actividad física, peso y uso de medicamentos. La glucosa fue significativamente menor en El Salvador que en Puerto Rico (123.6 vs 172.6 mg/dL; p = 0.0006), a pesar de suspender la metformina, coincidiendo con una mayor actividad física. No hubo diferencias en la dieta. Se requieren estudios más amplios.
Palabras clave: diabetes tipo 2; variabilidad glucémica; migración; salud
Introduction
Type 2 diabetes mellitus is characterized by insulin resistance and progressive beta-cell dysfunction, resulting in relative insulin deficiency and chronic hyperglycemia (Goyal et al., 2023). Many patients with type 2 diabetes have at least one complication, with cardiovascular disorders accounting for most of the morbidity and death in this patient population (Zheng et al., 2017). According to the Centers for Disease Control and Prevention (CDC, 2022a), other health complications include chronic kidney disease, nerve damage, foot problems, oral health, vision, hearing, and mental health. For these reasons, the rise in diabetes cases represents a global health risk. The International Diabetes Federation (IDF, 2023a) reported that about 537 million people are diagnosed with diabetes worldwide. These numbers are expected to rise by 200 million cases by 2040, demonstrating the significant impact of diabetes mellitus on global public health (Carrillo‐Larco et al., 2019). It is important to note that certain racial and ethnic groups have higher rates of prediabetes and T2DM. People who identify as Hispanic or Latino have a higher prevalence of type 2 diabetes (12%) compared to non-Hispanic White individuals (7%) (CDC, 2022b). Regardless of different customs, this statement applies to Hispanic Latino individuals in countries like Mexico, Puerto Rico, Cuba, South and Central America, and other Spanish-speaking cultures. However, the 12% figure for Latino or Hispanic groups is an average percentage. Estimates show that if one is of Puerto Rican descent, the risk of developing type 2 diabetes is approximately double that of someone of South American descent (CDC, 2022).
A comparison between the prevalence of diabetes in a Central American country, such as El Salvador, and in Puerto Rico supports this statement. Cases of diabetes in adults in Puerto Rico reached a total of 413,400 compared to El Salvador, with 291,500 cases. These numbers represent a staggering prevalence of diabetes: 20.1% of the island’s population as of 2021, compared to a country that doubles Puerto Rico’s population, such as El Salvador, with a prevalence of 7.1% (IDF, 2023a, 2023b). According to Puerto Rico’s Health Department (2021), more than 50% of the cases of diabetes on the island are T2DM. A different survey found that 79% of patients diagnosed with diabetes report having poor mental health, and 62% report having poor health quality (Puerto Rico’s Health Department, 2021). In addition to the bad quality of life evidenced by these surveys, the World Health Organization (WHO, 2017) also found that the two leading causes of death in Puerto Rico were ischemic heart disease and diabetes mellitus. These rates are alarming and hint at a deeper problem. T2DM is preventable with lifestyle modifications, such as maintaining a healthy body weight, eating a balanced diet, and exercising regularly. These same lifestyle factors can also contribute to diabetes management (Zheng et al., 2017). Understanding lifestyle changes that can improve diabetes management and outcomes is needed. Lifestyle factors include diet, weight, and physical activity (Flood et al., 2022). Observing patterns of an unhealthy lifestyle within a culture raises the question of a correlation with the high prevalence of diabetes in a country. Studies such as Pérez et al. (2015) have found that adults living in Puerto Rico’s metropolitan areas have mostly unhealthy nutritional status and dietary quality, evidenced by highly ranked unhealthy foods (such as sweets, sugary beverages, and fast foods) and low adherence to the recommended intakes of potassium, vitamin D, and high-quality food groups. Comparative dietary quality indicators suggest potential contextual differences between El Salvador and Puerto Rico; however, these comparisons should be interpreted cautiously, given methodological differences in measurement tools. In El Salvador, dietary quality was assessed using the Household Diet Quality Indicator (HDQI), which yielded a mean score of 63.5 out of 100, reflecting moderate dietary adequacy at the household level (Fuster et al., 2014). Notably, 79.3% of households presented both nutrient deficiencies and excesses, indicating persistent imbalances despite the overall score (Fuster et al., 2014). In contrast, diet quality among Puerto Ricans was evaluated using the Healthy Eating Index (HEI-2010), an individual-level measure aligned with U.S. dietary guidelines, which showed a median score of 58.7, with 19.6% classified as having poor diet quality and only 2% meeting criteria for a “good” diet (Lopez-Cepero et al., 2017). Importantly, the HDQI and HEI differ in their conceptual frameworks, scoring criteria, and levelsof analysis (household vs. individual), limiting direct numerical comparability. Therefore, while El Salvador’s mean HDQI score appears slightly higher than Puerto Rico’s median HEI score, these findings should not be interpreted as definitive evidence of superior diet quality, but rather as suggestive of contextual dietary differences that warrant further standardized cross-national investigation.
Rationale and Research Problem
Although the epidemiological burden of T2DM and its disproportionate impact on Hispanic and Latino populations have been well established, considerably lessattention has been given to how patterns of mobility influence day-to-day metabolic control. Given differences in diabetes prevalence and migration patterns across Hispanic and Latin American regions, understanding how circular migration may influence diabetes management is essential. The European Migration Network (2011) defines circular migration as “a repetition of legal migrations by the same person between two or more countries.” The focus of this case study is permanent migration and temporary return, where migrants have emigrated for good but return for temporary stays (Task Force on Measuring Circular Migration, 2017). Puerto Rico is not unfamiliar with this practice, as many residents travel between the island and the United States mainland for economic opportunities (Otterstrom & Tillman, 2013). Though Puerto Rico is considered an American territory, it is part of Latin America and possesses a strong cultural identity reflected in its dietary customs. This study examines short-term glycemic variation within a circular migration context. While prior research has examined migration in relation to healthcare access, stress, and disease prevalence, most studies evaluate migrant populations within a single host-country context rather than examining within-person metabolic changes across repeated migratory cycles. Circular migration is increasingly recognized as a social determinant of chronic disease management, particularly for T2DM. Migration involves transitions between environments, healthcare systems, food systems, and social networks, exposing individuals to shifting lifestyle and structural contexts that may influence metabolic stability and glycemic control (Ruiz Jiménez, 2025). Effective diabetes management depends on consistent self-care behaviors, including medication adherence, dietary regulation, and physical activity (American Diabetes Association [ADA], 2019; Hadziabdic et al., 2020). However, migrant populations often face barriers that weaken self-management, including limited disease knowledge and structural obstacles (Hadziabdic et al., 2020; Hjelm et al., 1999. Dietary transition further complicates management, as immigration has been associated with increased consumption of processed foods and reduced physical activity, contributing to obesity and T2DM progression (Ruiz Jiménez, 2025). Conversely, exposure to traditional dietary structures may influence glycemic variability differently. Despite these findings, there remains limited evidence examining short-term, within-person glucose variability during active circular migration between two sociocultural contexts. Most available research relies on cross-sectional prevalence data rather than longitudinal observation within the same individual across environmental transitions. Although higher T2DM prevalence among migrant populations has been documented (Cho et al., 2018; Hadziabdic et al., 2020; Montesi et al., 2016), the metabolic implications of repeated environmental transitions remaininsufficiently examined. This gap is particularly relevant in Puerto Rico, where diabetes is one of the two leading causes of death (World Health Organization, n.d.). T2DM is preventable and manageable through lifestyle modifications, including maintaining a healthy body weight, consuming a balanced diet, and engaging in regular physical activity. Because glycemic control depends heavily on consistent self-management behaviors, shifts in cultural, dietary, and structural environments may alter metabolic outcomes in ways that are not yet well understood. Investigating T2DM in relation to culturally embedded determinants such as diet, physical activity, and lifestyle habits is important for understanding how social and environmental contexts shape metabolic outcomes. Therefore, the central research question guiding this study is: How does circular migration between Puerto Rico and El Salvador influence short-term daily glycemic control in a patient with T2DM? This exploratory case study aims to examine whether observable differences in lifestyle context across two countries correspond with measurable changes in fasting glucose levels.
Hypothesis
It was hypothesized that fasting glucose levels would be significantly lower in El Salvador compared to Puerto Rico, and that this difference would coincide with higher levels of physical activity and a macronutrient distribution more closely aligned with recommended dietary guidelines. Specifically, it was anticipated that the subject would demonstrate increased daily step counts and a more balanced dietary intake in El Salvador, whereas residence in Puerto Rico would be associated with lower physical activity and a less balanced macronutrient profile. These contextual differences were expected to correspond with higher fasting glucose levels during the Puerto Rico observation period.
Methodology
The case study subject recorded daily logs of his glucose levels, measured in mg/dL, using his glucose monitor each morning. The dates and glucose values displayed on the monitor were included in the data tracked in this research. Additionally, the subject logged his food intake at several time points throughout the day in a nutritional diary using the app “MyFitnessPal.” The nutritional diary provided information such as daily caloric intake, macronutrient consumption, and total nutrient distribution. The participant wore a RedMi Smart Band 2 to track physical activity. MyFitnessPal also recorded the subject’s age, height, gender, and weight to calculate estimated caloric needs and macronutrient targets for body maintenance. This data was used to compare the patients’ daily caloric and macronutrient intake between the two countries. The study used the subject’s weight, measured at four time points during his trip to El Salvador, and compared it with the weight recorded upon his return to Puerto Rico. The data provided by the case study subject were entered into Excel tables and organized by week, recording carbohydrates, proteins, fats, physical activity, glucose levels, and weight. In addition, daily caloric intake and medication doses were recorded to allow contextual comparison between countries. This data was analyzed and graphed using Python (Google Colab) to compute descriptive statistics, between-country comparative analyses, and correlation measures. Descriptive statistical analyses were performed separately for El Salvador and Puerto Rico. Means, standard deviations (SD), and ranges (minimum–maximum) were calculated for fasting glucose levels, macronutrient intake, caloric consumption, and physical activity (steps) in each country. These statistics were used to compare central tendency and variability between contexts. To evaluate differences between countries, non-parametric Mann–Whitney U tests were conducted for fasting glucose, macronutrients, caloric intake, and physical activity, given the small sample size and non-normal distribution of daily observations. Spearman’s rank correlation analyses were performed within each country to assess associations between fasting glucose and lifestyle variables. To explore potential associations between lifestyle factors and glycemic control, Spearman rank correlation analyses were conducted between fasting glucose levels and daily carbohydrate intake, total caloric intake, and physical activity. Spearman’s correlation was selected, given the small sample size and the exploratory nature of the study. Given the single-subject design (n = 1), these analyses were considered descriptive and exploratory rather than inferential. Because multiple daily measurements were obtained from the same individual, observations are not fully independent. Therefore, nonparametric comparisons and correlation analyses should be interpreted as exploratory assessments of within-person variation rather than population-level inferential tests.
During the first week of the research conducted in Puerto Rico the participant did not wear his RedMi Smart Band 2 for the first four days. During the second week, the patient did not wear his physical activity tracker for three days, stating that he barely got out of bed during that period. The weight data for the second week of the study in El Salvador were not provided by the patient. Days with missing data were excluded from analyses involving those specific variables but retained for other available measures (using pairwise deletion). No experimental manipulation of medication doses, diet, fasting glucose measurements, or physical activity occurred during the study. The research relied exclusively on self-recorded and device-tracked data collected under naturalistic conditions. The study exclusively used voluntarily provided data by the patient. Only encrypted digital applications and technologies were used to record and analyze participants’ data, ensuringconfidentiality and patient safety. The participant was fully aware of the voluntary nature of this study and provided informed acknowledgment of the procedures and associated considerations. The primary outcome measured in this study was fasting glucose level (mg/dL). Additional contextual measures included daily caloric intake, macronutrient distribution (carbohydrates, proteins, and fats), physical activity quantified by average daily steps, body weight (kg), medication dosage (mg), and country of residence (El Salvador or Puerto Rico). These variables were analyzed descriptively to explore potential associations within the same individual across two distinct environmental contexts.
Data
Before presenting the figures, the data collected during the study are shown, organized according to key variables such as glucose levels, macronutrient consumption, physical activity, caloric intake, body weight, and medication use in both contexts (El Salvador and Puerto Rico). These tables enable a direct comparison of the patient’s conditions and serve as the foundation for the visual and statistical analyses presented in the following figures.
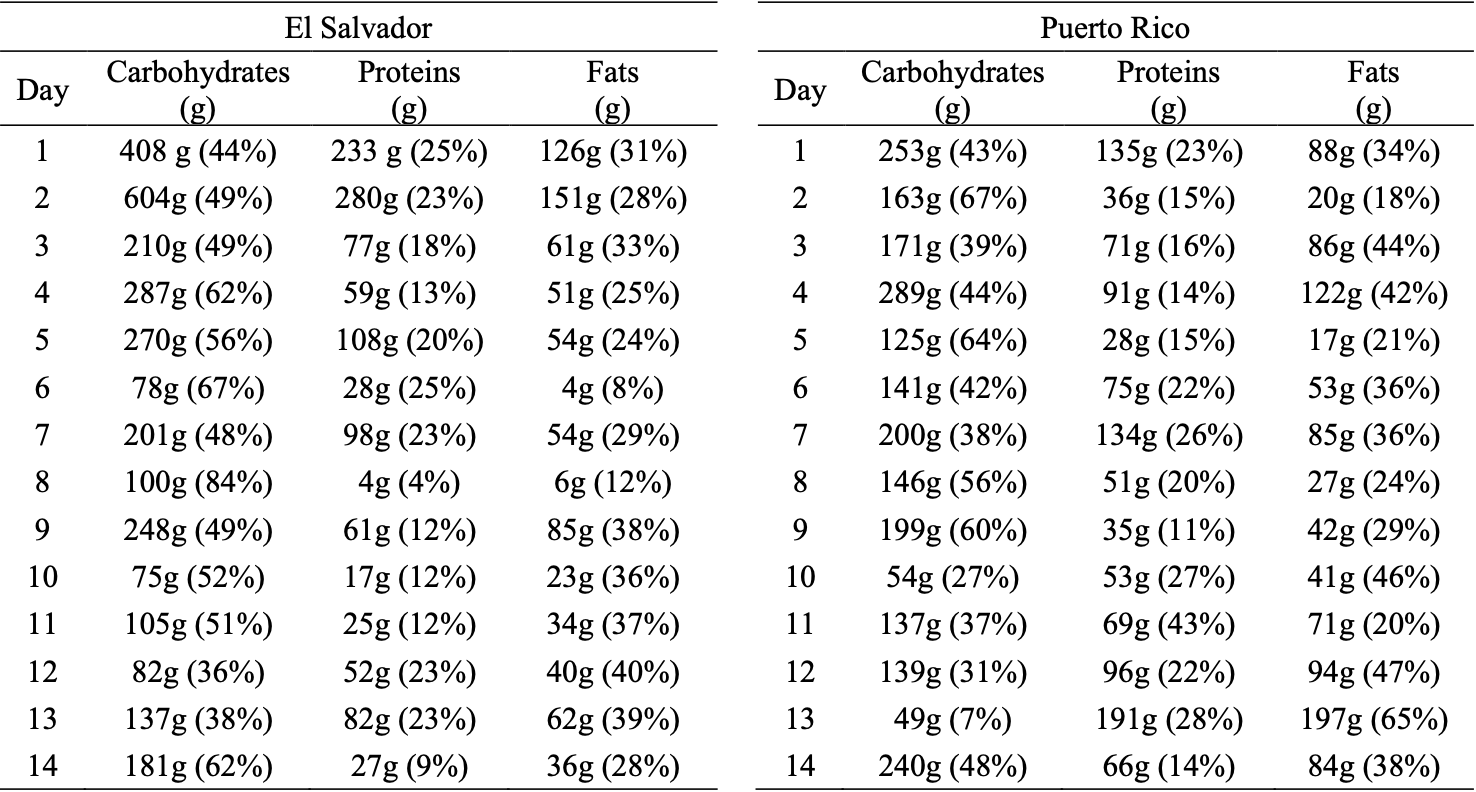
Table 1: Subject’s Daily Macronutrient Consumption
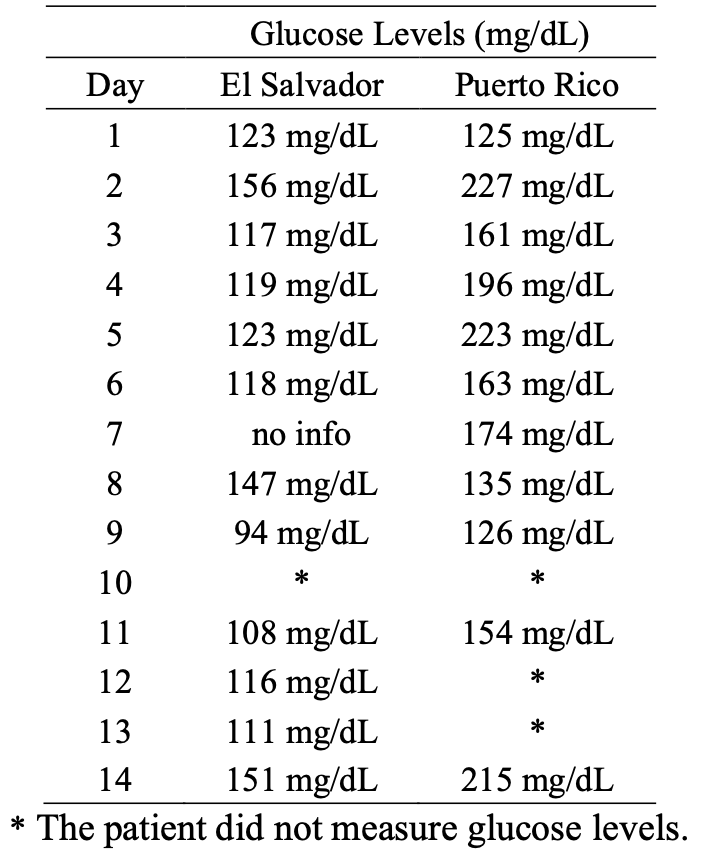
Table 2: Subject's Daily Glucose Levels in El Salvador and Puerto Rico
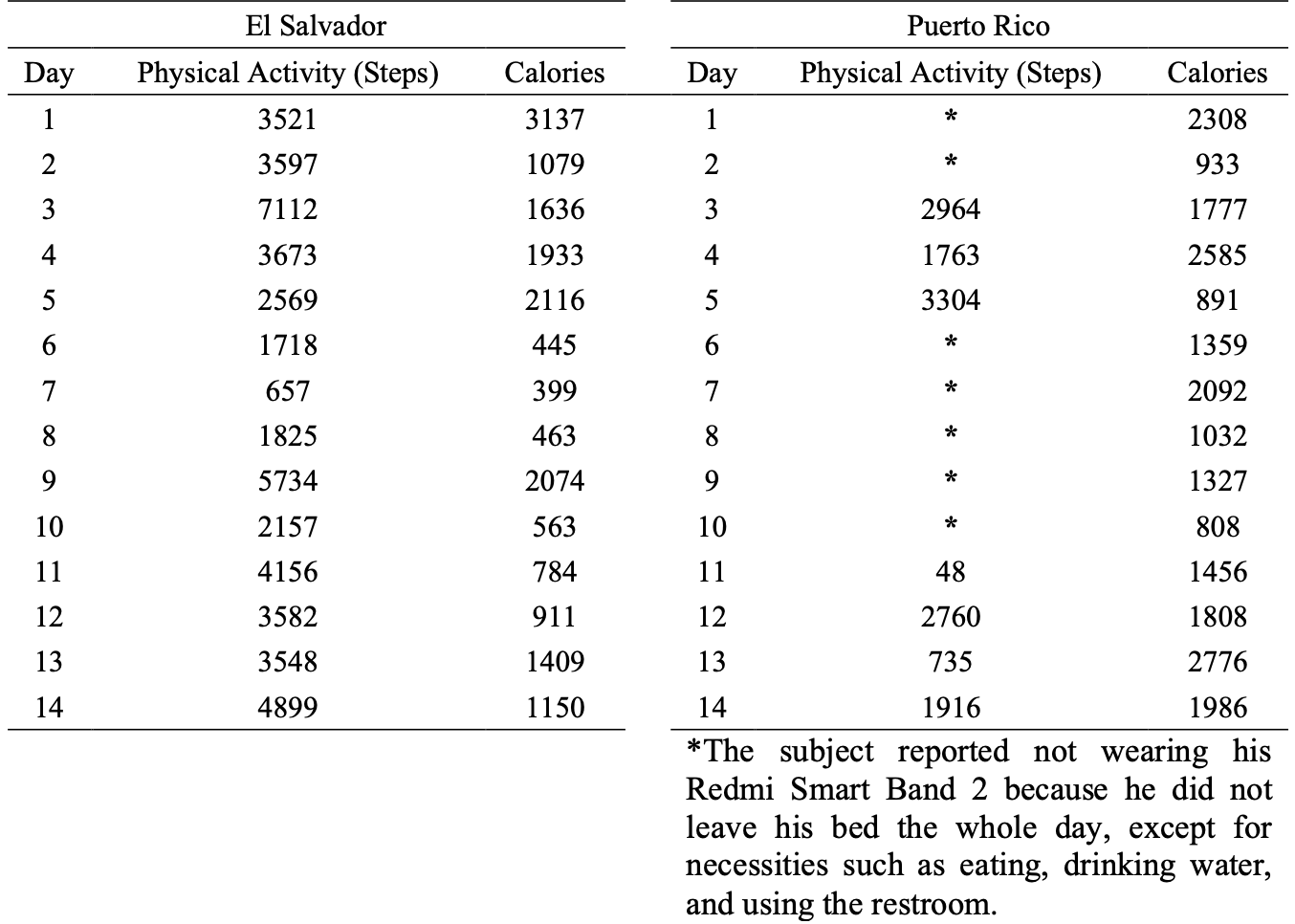
Table 3: Subject's Daily Physical Activity and Caloric Intake
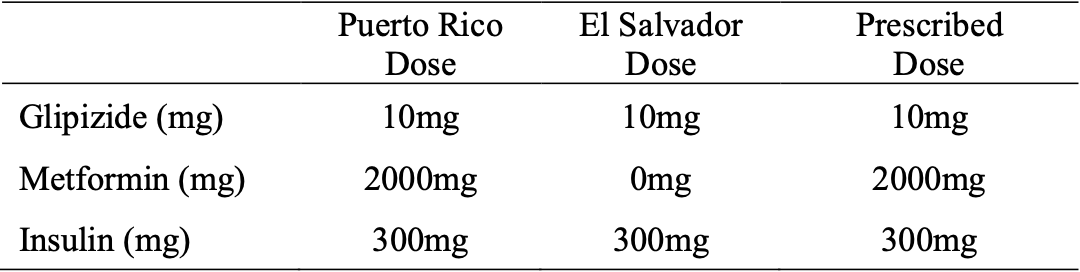
Table 4: Subject’s Prescribed Medication Doses and His Daily Ingestion
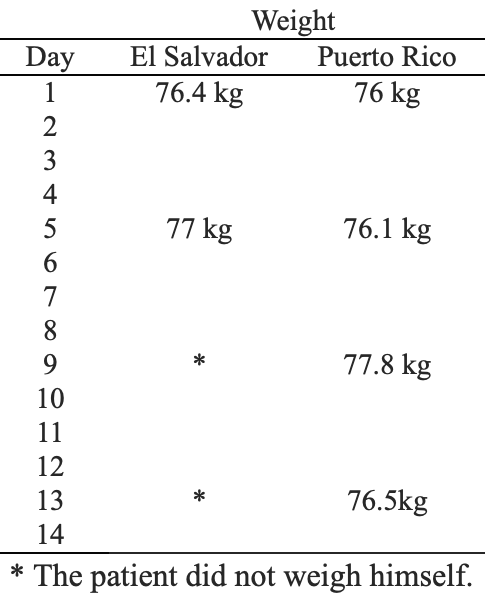
Table 5: Subject’s Weight
Data Analysis
Based on the data presented in the previous tables, the following figures were created to visualize differences between El Salvador and Puerto Rico in key variables, including glucose levels, physical activity, caloric intake, and macronutrient distribution. These graphical representations facilitate the identification of patterns and trends and complement the case study's comparative analysis.
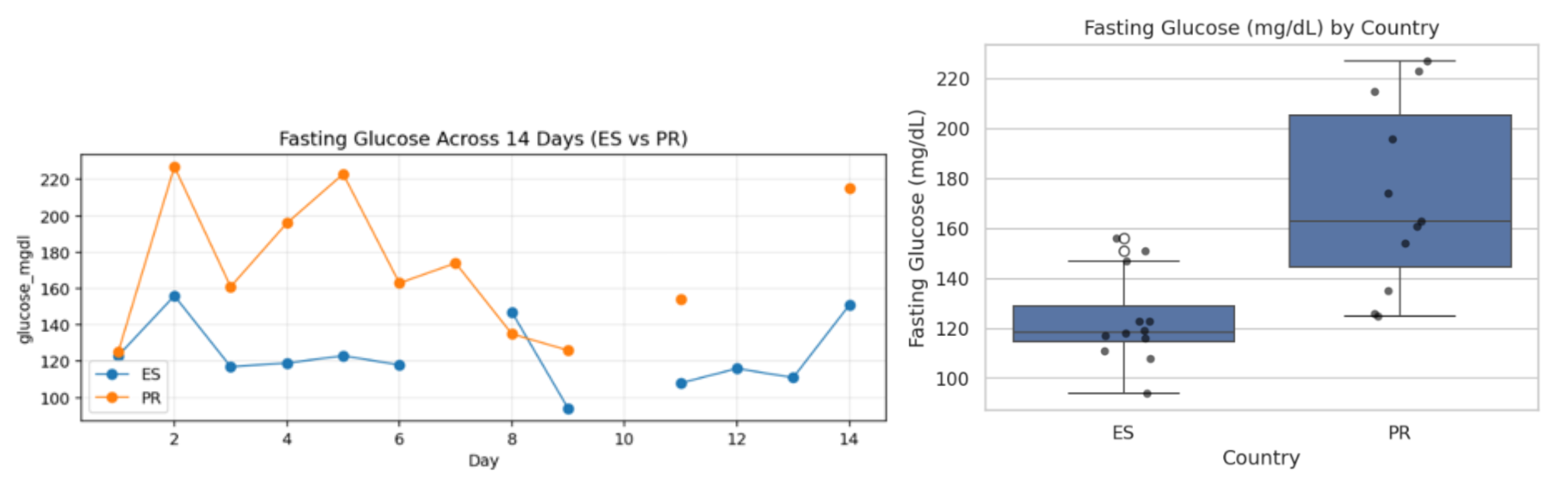
Figure 1: Fasting Glucose Levels in El Salvador and Puerto Rico
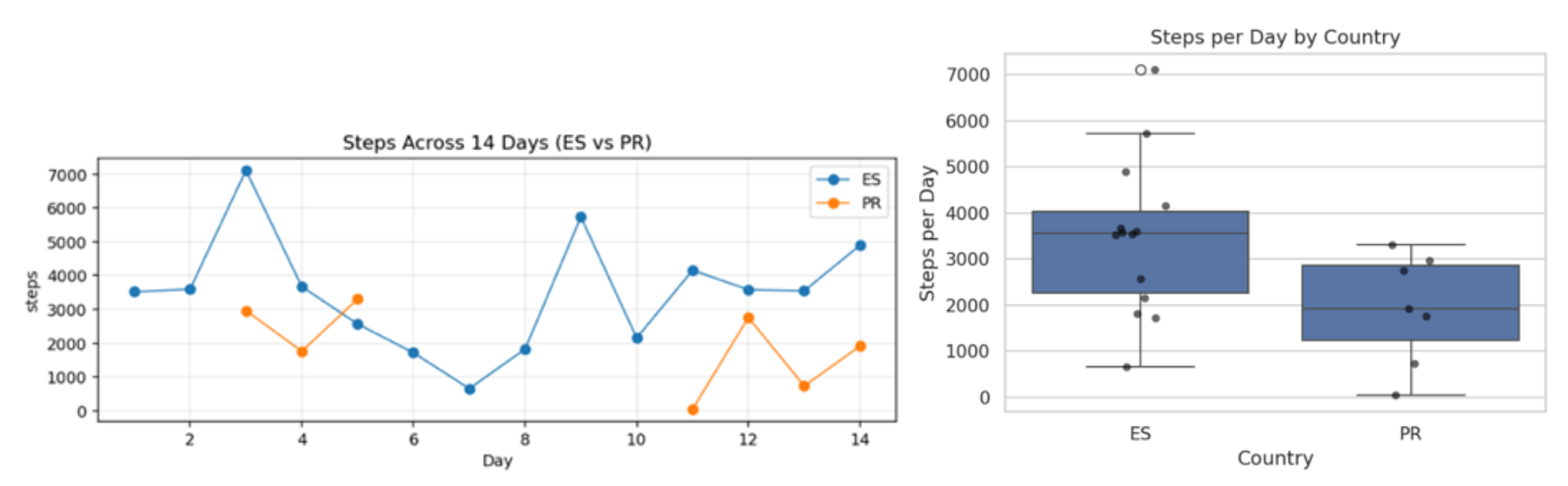
Figure 2: Physical Activity (Steps) in El Salvador and Puerto Rico
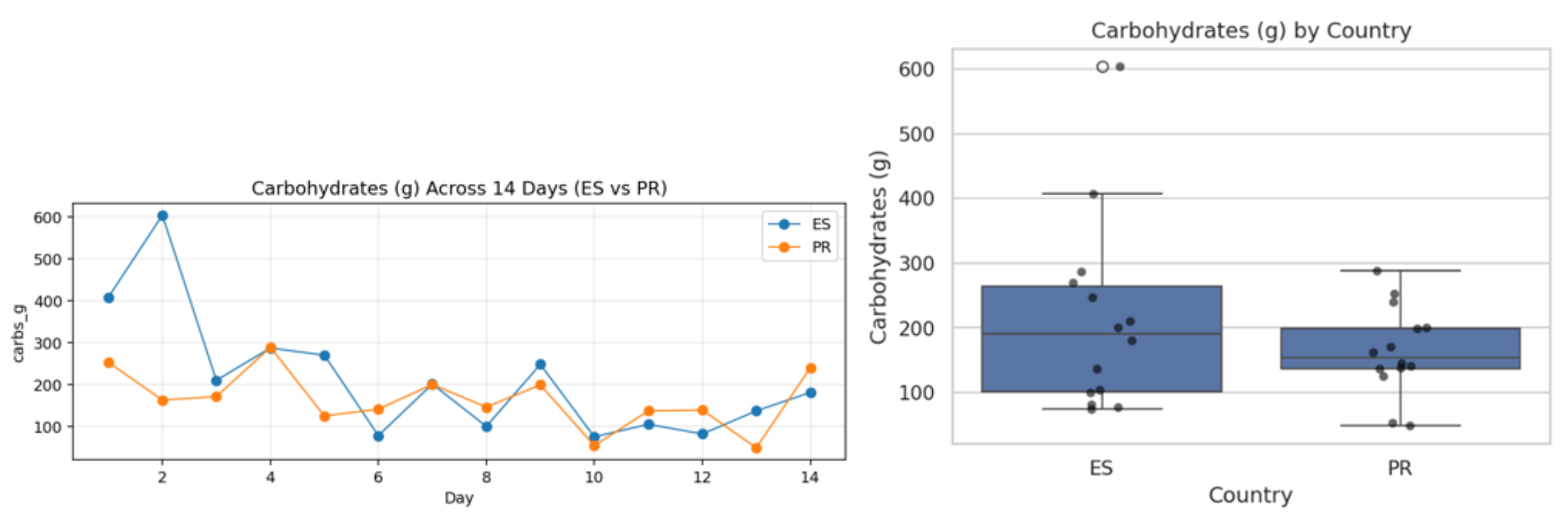
Figure 3: Carbohydrate Intake in El Salvador and Puerto Rico
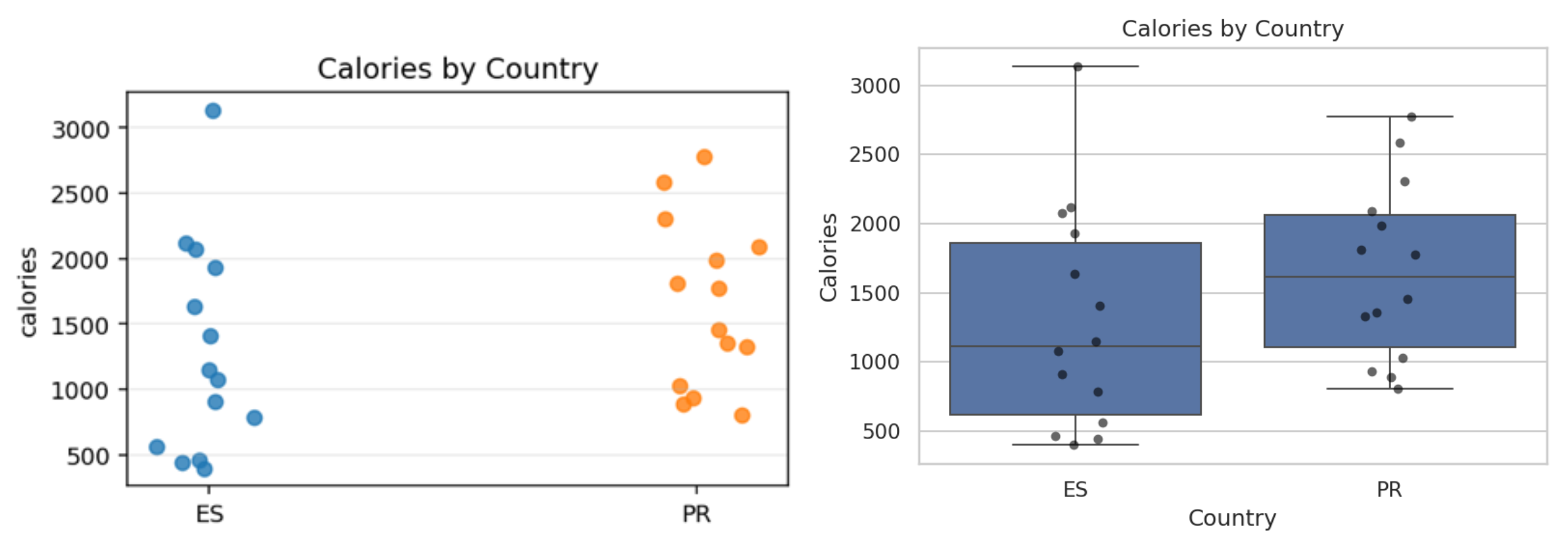
Figure 4: Caloric Intake in El Salvador and Puerto Rico
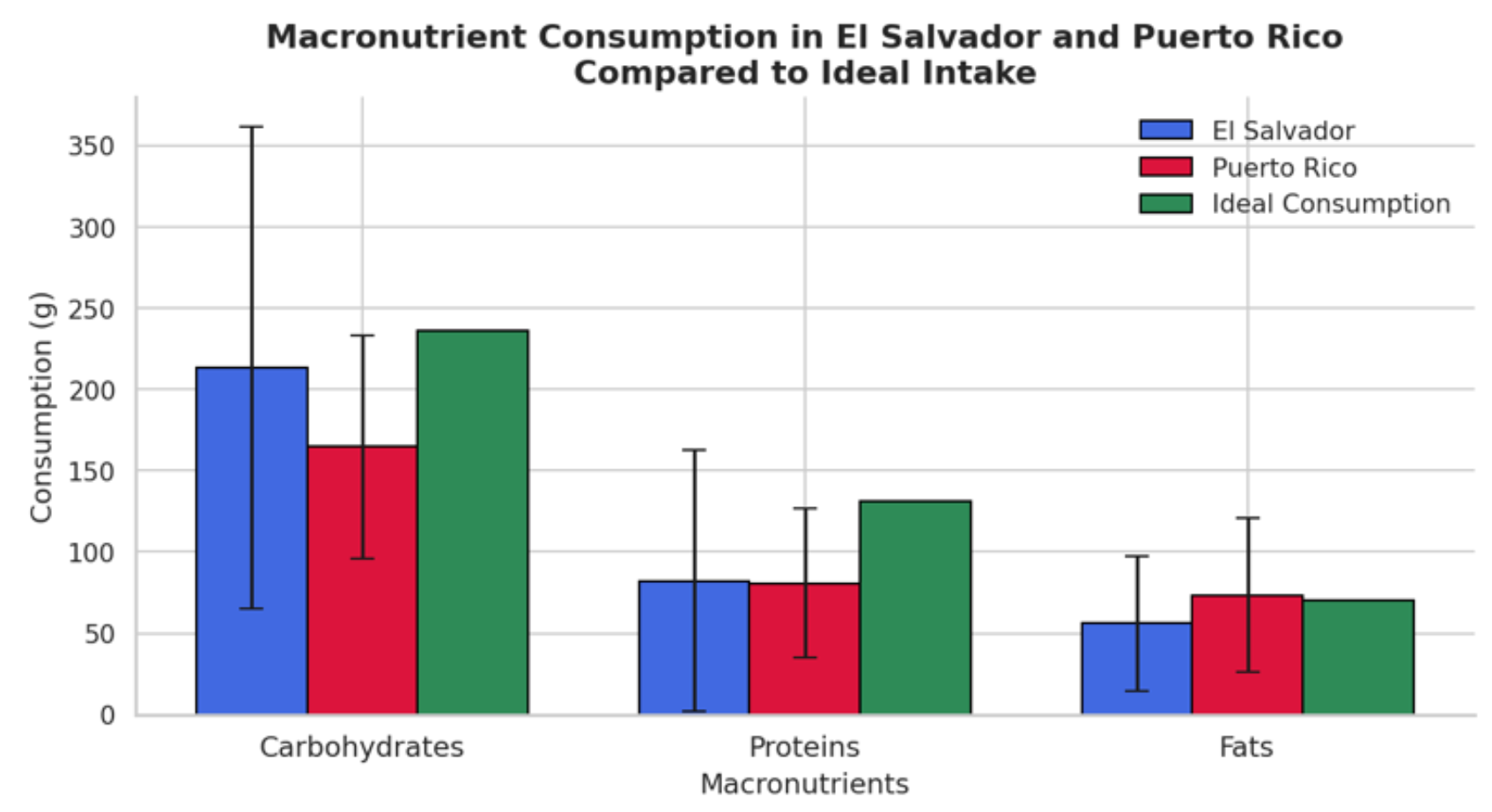
Figure 5: Mean Macronutrient Consumption Compared to Ideal Intake in El Salvador and Puerto Rico
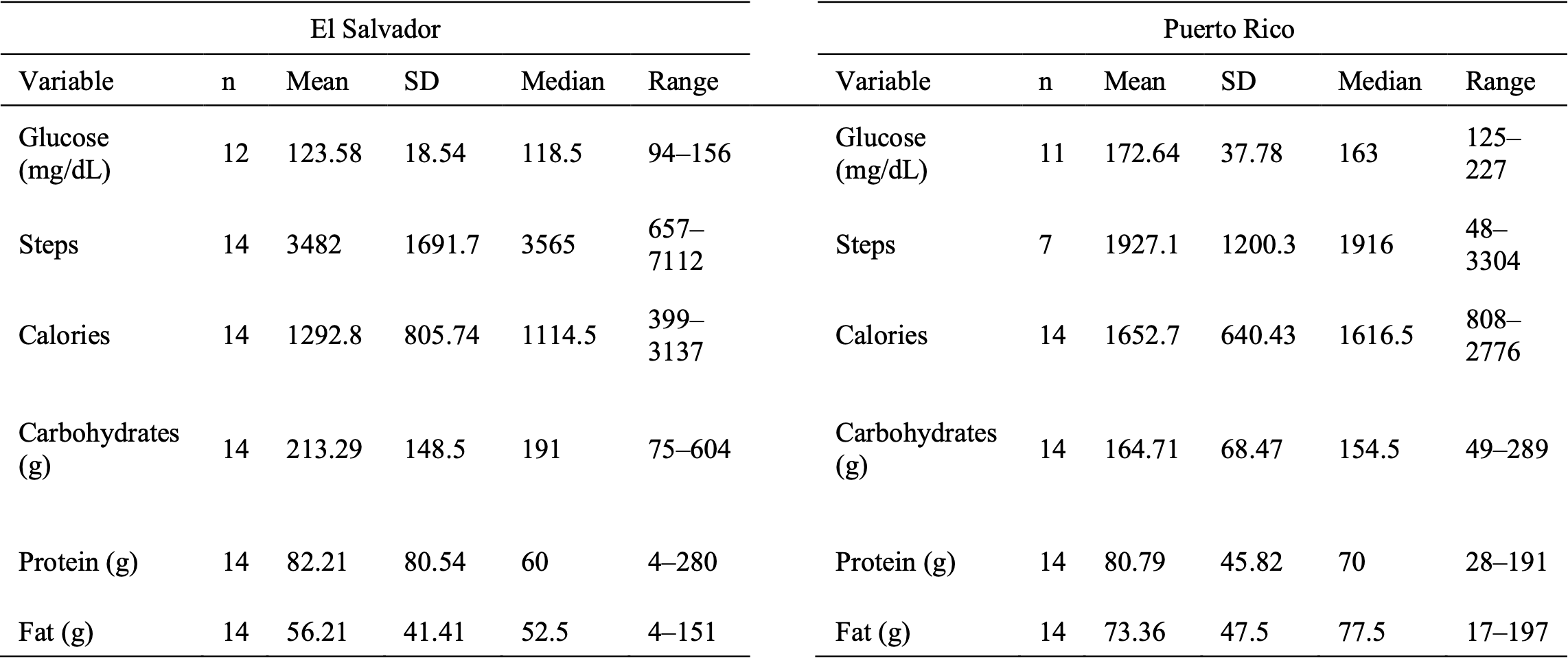
Table 6: Descriptive Statistics of Metabolic and Lifestyle Variables
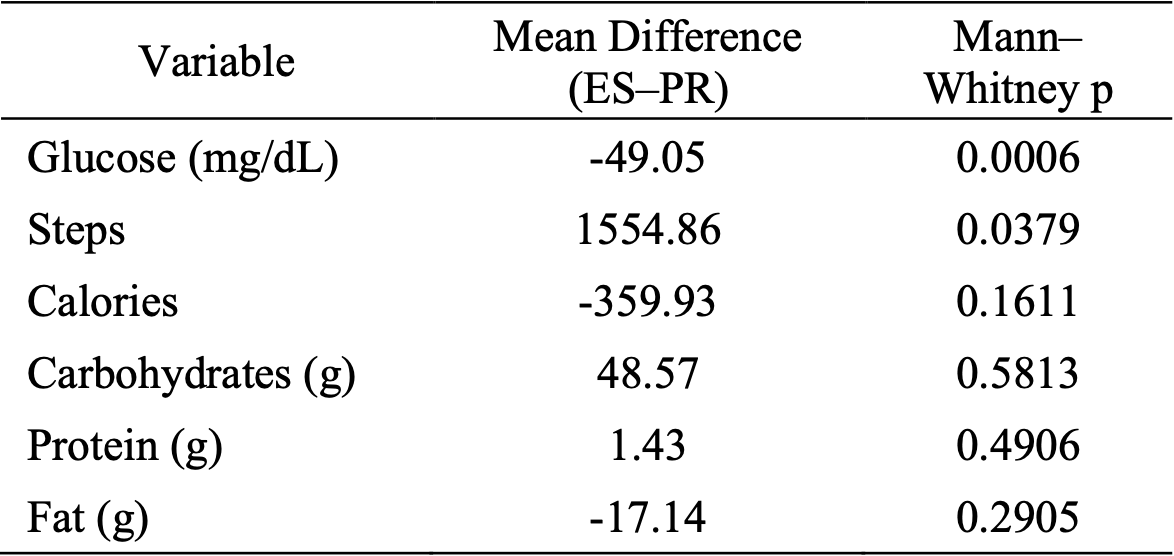
Table 7: Comparative Analysis of Metabolic and Lifestyle Variables Between El Salvador and Puerto Rico
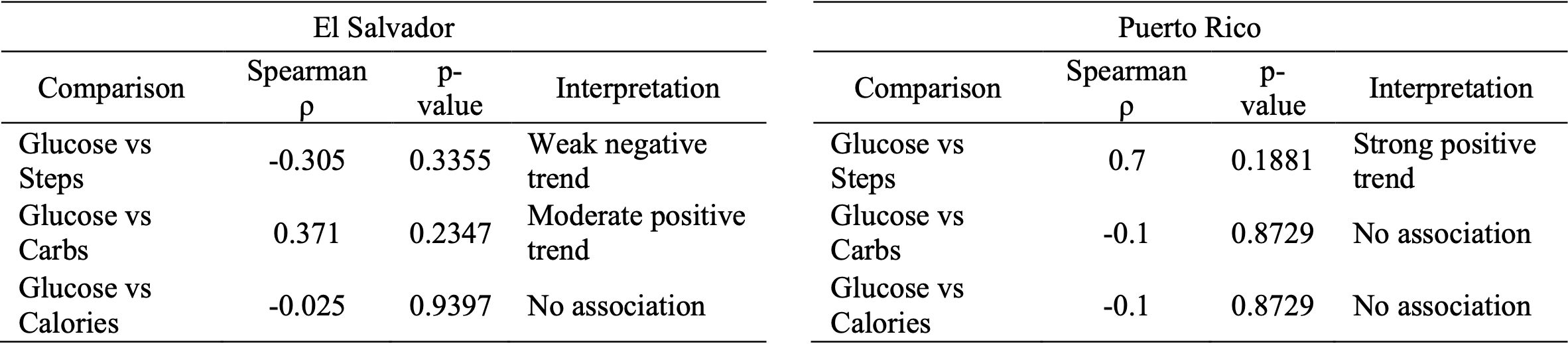
Table 8: Spearman Rank Correlation Coefficients Between Fasting Glucose and Lifestyle Variables
The subject had lower fasting glucose levels in El Salvador than in Puerto Rico (Figures 1a and 1b). Descriptive statistics summarized in Table 6 confirm this difference, with a mean glucose level of 123.58 mg/dL (SD = 18.54) in El Salvador compared to 172.64 mg/dL (SD = 37.78) in Puerto Rico. The Mann–Whitney U test indicated a significant within-person difference between observation periods (p = 0.0006). Glucose levels in El Salvador were more closely aligned with the recommended pre-meal range for patients with type 2 diabetes (80–130 mg/dL). Physical activity also differed between countries (Figures 2a and 2b). As shown in Table 6, the subject demonstrated higher daily step counts in El Salvador (Mean = 3482 steps, SD = 1691.68) compared to Puerto Rico (Mean = 1927.14 steps, SD = 1200.27). The comparative analysis in Table 7 confirms that this difference was statistically significant (p = 0.0379). When comparing macronutrient consumption between El Salvador and Puerto Rico (Figures 3 and 5), descriptive differences were observed. However, the statistical comparisons summarized in Table 7 revealed no significant differences in carbohydrate intake (p = 0.5813), protein intake (p = 0.4906), or fat intake (p = 0.2905). Caloric intake also did not differ significantly between countries (Figure 4; Table 7, p = 0.1611). Exploratory Spearman rank correlations conducted separately within each country (Table 8) did not reveal statistically significant associations between fasting glucose and daily carbohydrate intake, caloric intake, or physical activity. Although some directional trends were observed (e.g., a moderate positive trend between glucose and carbohydrate intake in El Salvador; ρ = 0.371), none reached statistical significance (all p > 0.05), reinforcing the exploratory nature of these within-country associations. Interestingly, in Puerto Rico, the correlation between fasting glucose and steps was positive (ρ = 0.70), contrary to the expected inverse relationship between physical activity and glucose levels. This unexpected direction may reflect the small number of valid step observations in Puerto Rico, missing tracker data, or day-to-day variability rather than a true physiological association. Notably, despite self-reported discontinuation of Metformin (Table 4) and maintenance of prescribed medication doses in Puerto Rico, fasting glucose levels remained significantly lower in El Salvador (Figures 1a–1b; Table 7). These findings suggest that contextual lifestyle factors—particularly physical activity—may have contributed to glycemic variability in this case.
Conclusions and Future Projections
The statistical comparisons summarized in Table 7 show that only fasting glucose levels and physical activity differed significantly between countries, while caloric and macronutrient intake did not. These findings are supported by Figures 1 and 2, which clearly display differences in fasting glucose levels and daily step counts across contexts. Although macronutrient distributions differed descriptively (Figures 3 and 5; Table 6), the lack of statistical significance advises cautious interpretation. While fasting glucose was notably lower in El Salvador, these results are based on repeated measurements within a single individual and should be viewed as exploratory rather than definitive evidence of group-level effects. Given the single-subject design (n = 1) and the non-independence of daily observations, the findings remain preliminary rather than causal. Nonetheless, the significant differences in Table 7, along with the trends seen in Figures 1 and 2, offer initial quantitative support for the idea that circular migration contexts might influence metabolic regulation. Future research should assess the effectiveness of antidiabetic medications across different lifestyle and environmental settings. In this case study, lower fasting glucose levels in El Salvador (Figure 1; Table 7) occurred despite discontinuing Metformin (Table 4), raising questions about how physical activity (Figure 2), dietary habits (Figures 3–5), stress, and sleep affect medication response. Understanding whether medication efficacy varies with lifestyle context could clarify if optimal glycemic control requires not only proper dosing but also supportive environmental factors. Long-term, controlled studies are necessary to determine whether the same medication regimens produce different metabolic outcomes depending on physical activity levels and dietary adherence. Combining behavioral and environmental factors with medication treatment may ultimately support more personalized and culturally sensitive diabetes management strategies for Latino populations.
References
American Diabetes Association. (2019). Check your blood glucose: Diabetes testing and monitoring. https://diabetes.org/living-with-diabetes/treatment-care/checking-your-blood-sugar
Carrillo-Larco, R. M., Aparcana-Granda, D. J., Mejia, J. R., Barengo, N. C., & Bernabe-Ortiz, A. (2019). Risk scores for type 2 diabetes mellitus in Latin America: a systematic review of population-based studies. Diabetic Medicine: A Journal of the British Diabetic Association, 36(12), 1573–1584. https://doi.org/10.1111/dme.14114
Centers for Disease Control and Prevention. (2022a, April 5). Diabetes risk factors. https://www.cdc.gov/diabetes/risk-factors/?CDC_AAref_Val=https://www.cdc.gov/diabetes/basics/risk-factors.html
Centers for Disease Control and Prevention. (2022b, June 20). Hispanic or Latino people and type 2 diabetes. https://minorityhealth.hhs.gov/diabetes-and-hispaniclatino-americans
Centers for Disease Control and Prevention. (2022c, November 3). Prevent diabetes complications. https://www.cdc.gov/diabetes/complications/?CDC_AAref_Val=https://www.cdc.gov/diabetes/managing/problems.html
Cho, N. H., Shaw, J. E., Karuranga, S., Huang, Y., da Rocha Fernandes, J. D., Ohlrogge, A. W., & Malanda, B. (2018). IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Research and Clinical Practice, 138, 271–281. https://doi.org/10.1016/j.diabres.2018.02.023
Departamento de Salud de Puerto Rico, División de Promoción para la Salud. (2021). Diabetes 2021. https://www.salud.pr.gov/CMS/DOWNLOAD/6792
European Migration Network. (2011). Temporary and circular migration: Empirical evidence, current policy practice and future options in EU Member States. https://emn.ie/files/p_201111110314492011_EMN_Synthesis_Report_Temporary_Circular_Migration_FINAL.pdf
Flood, D., Geldsetzer, P., Agoudavi, K., Aryal, K. K., Campos Caldeira Brant, L., Brian, G., Dorobantu, M., Farzadfar, F., Gheorghe-Fronea, O., Gurung, M. S., Guwatudde, D., Houehanou, C., Jorgensen, J. M. A., Kondal, D., Labadarios, D., Marcus, M. E., Mayige, M., Moghimi, M., Norov, B., … Manne-Goehler, J. (2022). Rural-urban differences in diabetes care and control in 42 low- and middle-income countries: A cross-sectional study of nationally representative individual-level data. Diabetes Care, 45(9), 1961–1970. https://doi.org/10.2337/dc21-2342
Fuster, M., Houser, R. F., Messer, E., de Fulladolsa, P. P., Deman, H., & Bermudez, O. I. (2014). Household-level dietary quality indicator for countries in nutritional transition: Application to vulnerable communities in El Salvador. Public Health Nutrition, 17(3), 529–536. https://doi.org/10.1017/S1368980013000426
Goyal R., Singhal M., & Jialal I. (2026). Type 2 Diabetes. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK513253/
Hadziabdic, E., Pettersson, S., Marklund, H., & Hjelm, K. (2020). Development of a group-based diabetes education model for migrants with type 2 diabetes, living in Sweden. Primary Health Care Research & Development, 21, e50. https://doi.org/10.1017/S1463423620000493
Hjelm, K., Bard, K., Nyberg, P., & Apelqvist, J. (2003). Religious and cultural distance in beliefs about health and illness in diabetic women of different originsliving in Sweden. International Journal of Nursing Studies, 40, 627–43. https://doi.org/10.1016/S0020-7489(03)00020-8
International Diabetes Federation. (2023a). El Salvador. https://idf.org/our-network/regions-and-members/south-and-central-america/members/el-salvador/
International Diabetes Federation. (2023b). Puerto Rico. https://idf.org/our-network/regions-and-members/south-and-central-america/members/puerto-rico/
López-Cepero, A., Valencia, A., Jiménez, J., Lemon, S. C., Palacios, C., & Rosal, M. C. (2017). Comparison of dietary quality among Puerto Ricans living in Massachusetts and Puerto Rico. Preventing Chronic Disease, 14, E51. https://doi.org/10.5888/pcd14.160439
Montesi, L., El Ghoch, M., Brodosi, L., Calugi, S., Marchesini, G., & Dalle Grave, R. (2016). Long-term weight loss maintenance for obesity: a multidisciplinary approach. Diabetes, Metabolic Syndrome and Obesity, 9, 37–46. https://doi.org/10.2147/DMSO.S89836
Otterstrom, S. M., & Tillman, B. F. (2013). Income change and circular migration: the curious case of mobile Puerto Ricans, 1995-2010. Journal of Latin American Geography, 12(3), 33–57. https://www.proquest.com/scholarly-journals/income-change-circular-migration-curious-case/docview/1449153891/se-2
Pérez, C. M., Soto-Salgado, M., Suárez, E., Guzmán, M., & Ortiz, A. P. (2015). High prevalence of diabetes and prediabetes and their coexistence with cardiovascular risk factors in a Hispanic community. Journal of Immigrant and Minority Health, 17(4), 1002–1009. https://doi.org/10.1007/s10903-014-0025-8
Ruiz Jiménez, A. B. (2025). Immigration and diabetes: A little-known reality. Diabetes, (91). https://www.revistadiabetes.org/wp-content/uploads/Immigration-and-Diabetes.-A-little-known-reality.pdf
World Health Organization. (2017). Country details: Puerto Rico. Mortality database. https://platform.who.int/mortality
Zheng, Y., Ley, S. H., & Hu, F. B. (2018). Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nature Reviews. Endocrinology, 14(2), 88–98. https://doi.org/10.1038/nrendo.2017.151
Esta obra está bajo una licencia de Creative Commons Reconocimiento-NoComercial 4.0 Internacional.